Medical Emergency Departments serve as a main entry point for patients into hospitals, and the team, the core of which is formed by doctors and nurses needs to make sense of and respond to the constant flux of information.
This requires sense-making, communication, and collaborative operational decision-making.
The study’s main aim was to explore how collective, interprofessional sense-making occurs in the emergency department. Collective sense-making is deemed a precursor for adaptive capability, which, in turn, promotes coping in a dynamically changing environment.
The study did demonstrate an operational disconnect between doctors and nurses caused by asymmetric information, disjointed decision-making approaches, differences in habitual communication styles, and a lack of shared feedback loops. By cultivating their varied sense-making experiences into one integrated operational foundation with stronger feedback loops, interprofessional teams’ adaptive capability and operational effectiveness […] can be improved.
SenseMaker surveys where used. These start with an elicitation question, prompting participants to tell a short descriptive story. The micro-narratives (short descriptive stories) provide more sensemaking context than structured narratives. For this study the prompting question presented participants with an interruption, the nature of which they could choose and disclose.
After sharing their story, participants are led through a series of specialised questions, called signifiers, that allow them to self-analyse their story within the pre-designed framework. The short descriptive story and signifier data are captured in a common database that visually displays data for further analysis. The software allows switching between quantitative (signifier) and qualitative (descriptive story) data during interpretation, enabling more deeply nuanced analyses.
The results focused on four aspects of sense-making, namely views on the availability of information, the consequences of decisions (actions), assumptions regarding appropriate action, and preferred communication methods. These processes enable (or are required for) adaptive capability.

This map combines the responses to two survey questions presented in a dyad format. Dyads have two extremes on a linear scale, with one extreme indicating the underlying construct to be completely absent and the other extreme presenting the construct in excess. This may appear similar to other commonly used linear scales, but the difference is that the preferred state is somewhere between the two extremes
The first dyad asked (x-axis): In your story, the consequence of the decisions that had to be made in the ED was. . . [and the extremes were: blindingly obvious // confusing and uncertain].
The second dyad asked (y-axis): The availability of the required information was. . . [with the extremes being: too little, too late, too hard to find // too much, too early, swamped with it.]
The three clusters identified in above figure are:
Top left: Feeling swamped with information, yet the consequence of the decision is obvious
Top right: Feeling swamped with information, yet confused about the consequence
Bottom left: Enough information and obvious consequence of the decision
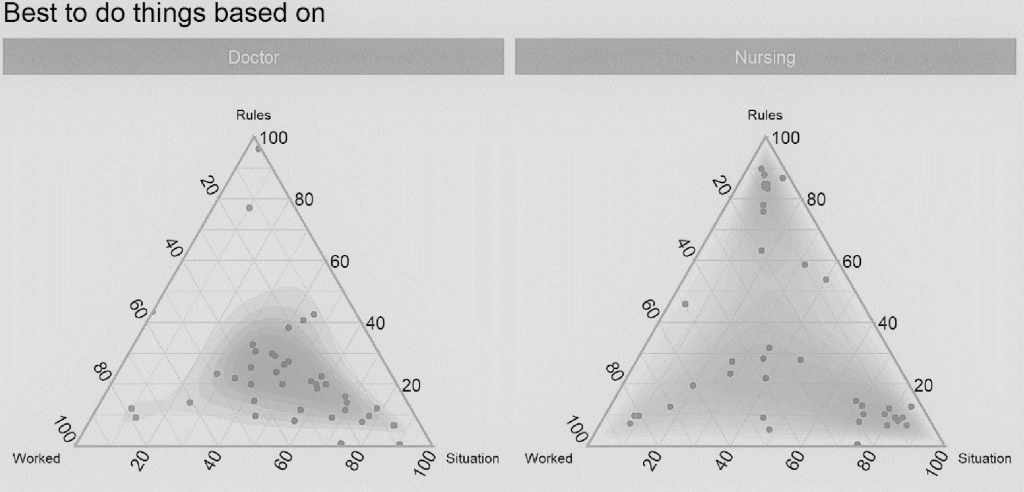
The interior of a triad represents the relative proportions of the three corner variables. The participant places a dot anywhere inside the triangle to demonstrate how the three variables at the corners trade off against each other.
Storytellers who placed a dot in the middle of the triad indicated the three corners are weighted equally, implying that the best course of action was contextual. Otherwise, there was a noticeable difference in what doctors and nurses felt would constitute appropriate action. The nurses (right-side triad) were divided, with clustering at ‘following the rules and policies’ or
‘according to the situation’, whereas doctors were more likely to act ‘according to the situation’.
This study contributes empirical knowledge as most studies done in EDs are focused one discipline or on a singled-out process condition. Theoretically the study adds insights into how sense-making occurs within a dynamic interprofessional setting and the findings/patterns emerged.
The SenseMaker tool provides unique opportunity to explore the human dynamics within complex systems . Advantages of using the method includes the ability to merge qualitative and quantitative data for nuanced analysis, the distance created between the researcher and interpretation of data to reduce bias, and the broad elicitation question permits a wide range of stories and interpretations by the participants.
Adaptive capability is situated at the operational level and can be amplified by improving interprofessional sense-making. Doctors’ and nurses’ different conditioning, perspectives and priorities present an untapped sense-making opportunity that should be exploited.
EDs are recommended to adopt an integrated approach for dealing with information, communication, and feedback loops. This means integrating formal operational structures, e.g., one set of shared operational rules and policies.
Special attention should also be paid to promote interprofessional communication practices that are frequent, timely, accurate, and sent via focused channels. Redesigning communication systems to allow reciprocal horizontal relationships would also improve knowledge management
